The Melghat region of Maharashtra, comprising the Dharani and Chikhaldara blocks in Amravati district, is home to a significant tribal population. Despite its picturesque landscapes and rich biodiversity, the area faced alarming maternal and child health challenges for decades. High infant mortality rate (IMR), maternal mortality rate (MMR), and malnutrition were persistent issues, exacerbated by cultural superstitions, language barriers, and the region’s difficult terrain. Recognising the urgency, the district administration, led by IAS Saurabh Katiyar (2016 batch, Maharashtra cadre), District Collector of Amravati, initiated “Mission 28” in 2022, a targeted program aimed at improving maternal and child health outcomes.
“Due to sustained efforts of Health and ICDS departments, IMR, MMR, and institutional deliveries are now nearly equal to the state average. The entire administration is committed to reducing child and maternal mortality in the Melghat region,” IAS Saurabh Katiyar shared with Indian Masterminds. This vision has been instrumental in driving the campaign’s success.
IDENTIFYING THE CHALLENGES
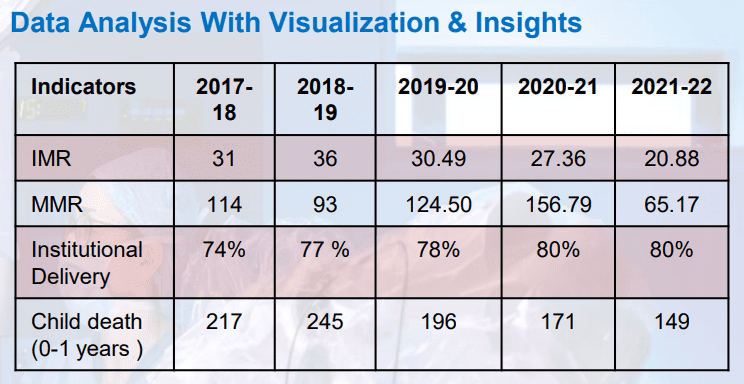
A comprehensive pre-project analysis highlighted the gravity of the health crisis in Melghat. In 2018-19, the IMR was 36, and the MMR stood at 87. Approximately 70% of infant deaths occurred within the first month of life, and 60% of these deaths happened at home due to limited institutional deliveries. The prevalence of severe acute malnutrition (SAM) and moderate acute malnutrition (MAM) further compounded the problem. Premature deliveries accounted for nearly 30% of the annual 7,000 births, resulting in low-birthweight babies vulnerable to septicaemia, pneumonia, and other diseases. Cultural superstitions, combined with the linguistic barriers posed by the local Korku language, discouraged many families from seeking medical care.

MISSION 28
Launched in 2022, Mission 28 focused on a critical 56-day period around childbirth—28 days before delivery and 28 days after delivery. This innovative strategy involved close monitoring of pregnant women and lactating mothers, leveraging grassroots healthcare networks and infrastructure improvements.
KEY INTERVENTIONS
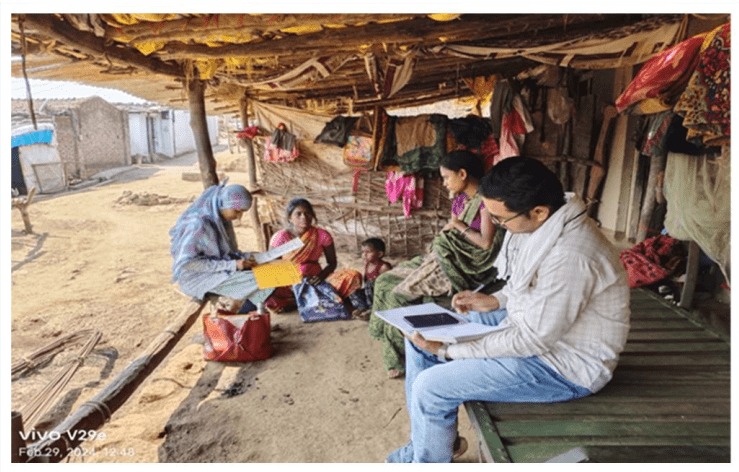
Community leaders, including Gram Sevaks and teachers, were mobilised to address superstitions and encourage healthcare access. Counselling sessions were conducted in the local Korku language by specially trained counsellors to build trust and improve communication. Comprehensive training programs were organised for ASHA workers, Anganwadi workers, and other healthcare staff. These sessions were staggered over three days to prevent fatigue. Regular workshops emphasised the importance of institutional deliveries and neonatal care.
Nutritional rehabilitation centres, blood banks, and child treatment centres were established in primary health centres. Specialised doctors visited critical villages for 15 days each month to provide necessary medical support. Dedicated ambulances for pregnant women and neonatal care ensured timely assistance. High-risk pregnancies were identified and monitored by specialised medical teams.
Three colour-coded cards were introduced for systematic tracking: yellow for y care, saffron for postnatal care up to 28 days, and green for neonatal care up to 28 days. Helplines were established for pregnant women to access immediate medical advice. Wage loss compensation was provided under the Manav Vikas scheme to encourage institutional deliveries.

IMPACT AND RESULTS
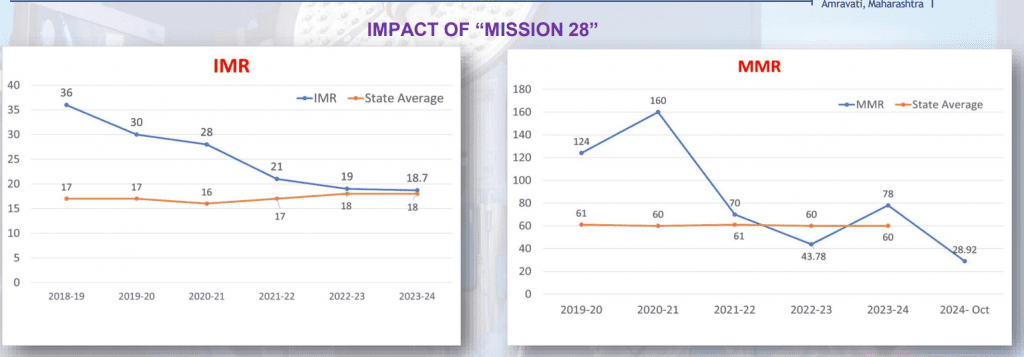
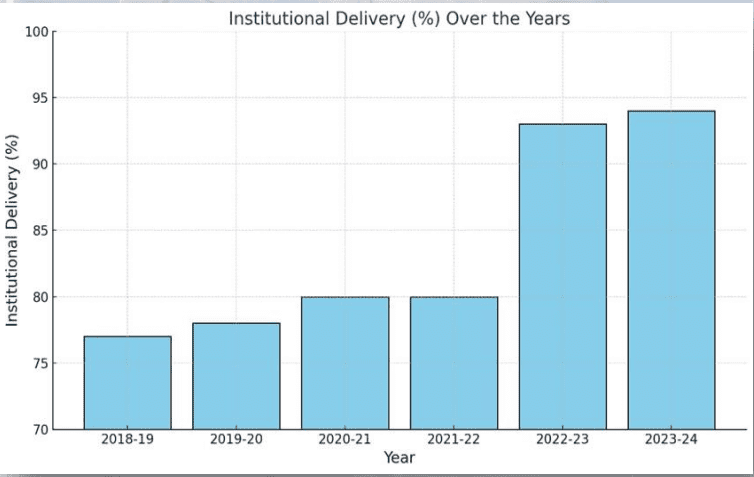
The implementation of Mission 28 has brought about a transformational change in maternal and child health indicators in Melghat. IMR decreased from 36 in 2018-19 to 19.98 in 2023-24. MMR dropped significantly from 93 to 28.92 during the same period. The rate of institutional deliveries rose from 77% in 2018-19 to 94% in 2023-24, ensuring safer childbirth practices. Infant deaths reduced from 245 in 2018-19 to 128 in 2023-24. These improvements have brought the region’s health indicators closer to the state average, showcasing the effectiveness of the initiative.
BEST PRACTICES
Mission 28 provides valuable insights into addressing health challenges in underserved regions. Addressing cultural and linguistic barriers through community involvement and local language counselling proved vital. Training and mobilising ASHA and Anganwadi workers ensured effective last-mile delivery of healthcare services.
The initiative’s cost-effective design leveraged existing resources, making it replicable in similar regions. Monthly reviews and the use of colour-coded cards ensured the campaign remained dynamic and responsive to community needs. Acknowledging the efforts of healthcare workers boosted morale and maintained high performance levels.

THE ROAD HEAD
Mission 28 has not only transformed the health landscape of Melghat but also set a precedent for other tribal and rural regions grappling with similar issues. Its success underscores the importance of innovative, community-driven approaches to public health. As IAS Saurabh Katiyar aptly stated, the commitment of the administration and the collaborative efforts of health and ICDS departments have been key to achieving these milestones.
With sustained efforts and continued focus, Melghat is poised to become a model for maternal and child health interventions, inspiring similar transformations across the country.